Melasma vs Hyperpigmentation: How Hyperpigmentation and melasma treatment is done
Table of Contents
- Introduction to Melasma and Hyperpigmentation
- What Is Hyperpigmentation?
- What Is Melasma?
- Melasma vs Hyperpigmentation: Key Differences
- How to Identify Melasma at Home
- How to Identify Regular Hyperpigmentation
- What Is PIH and How Is It Different?
- Why Melasma Keeps Coming Back
- How to Treat Hyperpigmentation Faster
- How to Treat Melasma Safely
- Melasma vs Hyperpigmentation: Which One Fades Faster?
- Science-Backed Insights on Pigmentation
- Final Thoughts
- References
- FAQS
Pigmentation is one of the most common skin concerns. Yet few people know whether they’re dealing with melasma, regular hyperpigmentation, or another form of discoloration. Many online descriptions sound similar, and skincare products often use the same language for every type of dark spot.
If you’re new to pigmentation, read our full guide on the basics: What Is Skin Pigmentation?


But Melasma vs Hyperpigmentation are not the same. They have different causes, patterns, triggers, and treatment responses. Confusing one for the other can slow your progress or cause irritation that makes pigmentation worse.
This science-backed guide explains the differences clearly. You’ll learn how to identify each condition, why they form, and the best hyperpigmentation and melasma treatment options supported by current dermatology research.
What Is Hyperpigmentation?
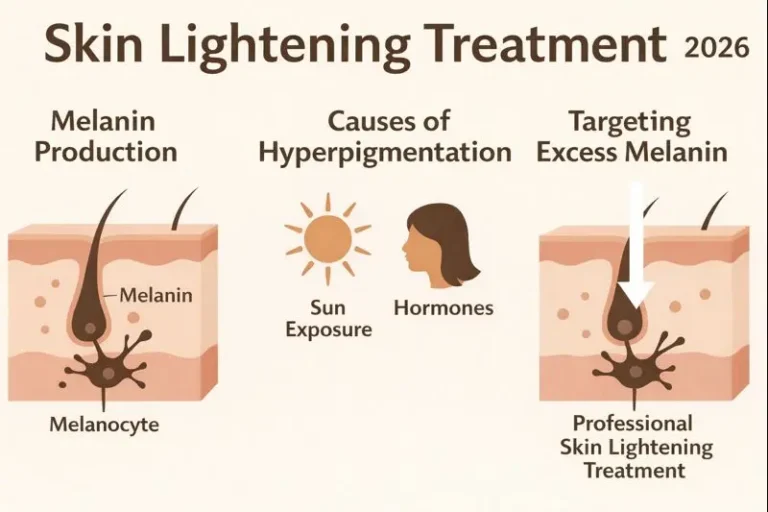
Hyperpigmentation is an umbrella term for any darkening of the skin. It can appear as spots, patches, or uneven tone. It happens when melanocytes produce too much melanin. This excess pigment collects in specific areas, making the skin look darker.
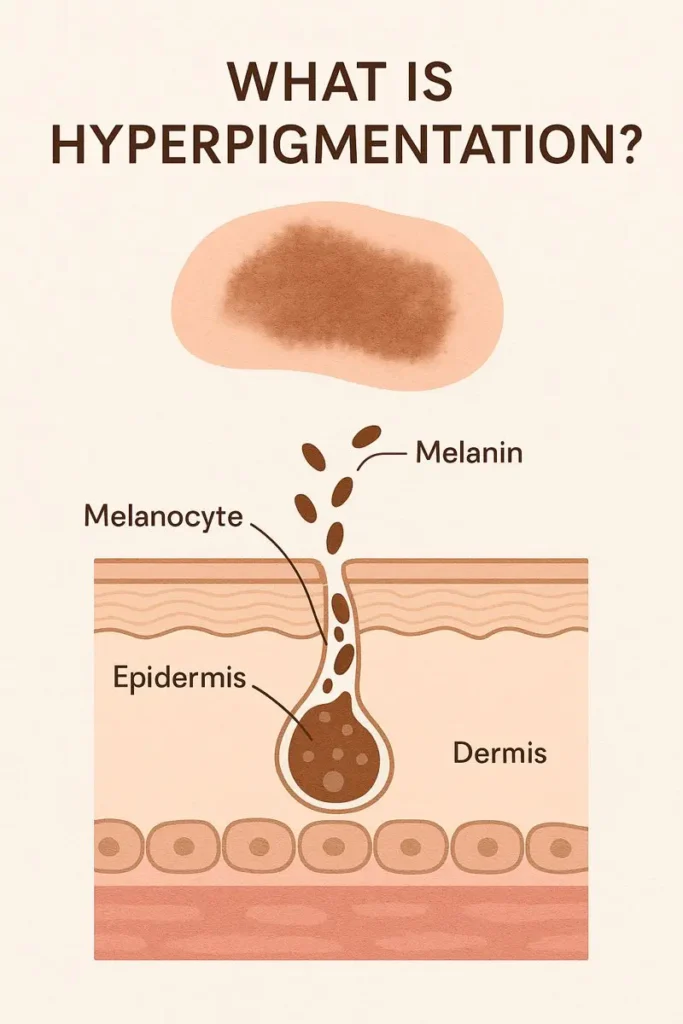
To understand how hyperpigmentation starts, it helps to know how melanin production works.
Read: What Is Skin Pigmentation? Causes, Types & Common Myths
Hyperpigmentation has many causes. The most common include sun exposure, acne, skin injury, hormones, and inflammation. It affects all skin types, but deeper tones often produce more melanin in response to irritation. This makes hyperpigmentation more visible and more persistent.
Hyperpigmentation types include sunspots, age spots, freckles, post-inflammatory hyperpigmentation (PIH), and dark marks after acne.
The good news: hyperpigmentation responds well to consistent topical treatments and sun protection, especially when caught early.
What Is Melasma?
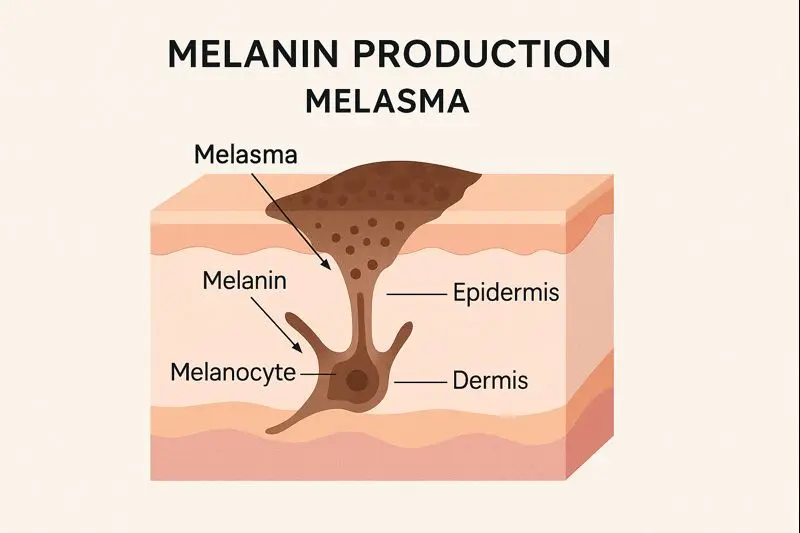
Melasma is a specific type of pigmentation that forms symmetrical patches, usually on the cheeks, forehead, upper lip, or chin. It is strongly hormone-driven. This makes it different from regular hyperpigmentation, which usually comes from external triggers like sun or acne.
Melasma is also persistent. It tends to recur even after treatment if triggers aren’t controlled. This is why dermatologists often call melasma a chronic condition that requires long-term management rather than a quick cure.
It is far more common in women, especially during pregnancy, with hormonal contraceptive use, or in people with Fitzpatrick skin types III–VI (including South Asian, Middle Eastern, Latin American, and Mediterranean skin).
Melasma vs Hyperpigmentation: The Core Differences
Understanding melasma vs hyperpigmentation comes down to five major distinctions: cause, appearance, depth, triggers, and treatment response.
1. Cause
Hyperpigmentation usually forms from:
- Sun damage
- Acne
- Injuries
- Irritation
- Heat
- Allergic reactions
- Friction
Melasma forms from:
- Hormonal changes
- UV exposure
- Heat
- Genetic predisposition
Hormones play the biggest role in melasma. This is why melasma flares during pregnancy, after starting birth control, or when hormones fluctuate.
2. Appearance
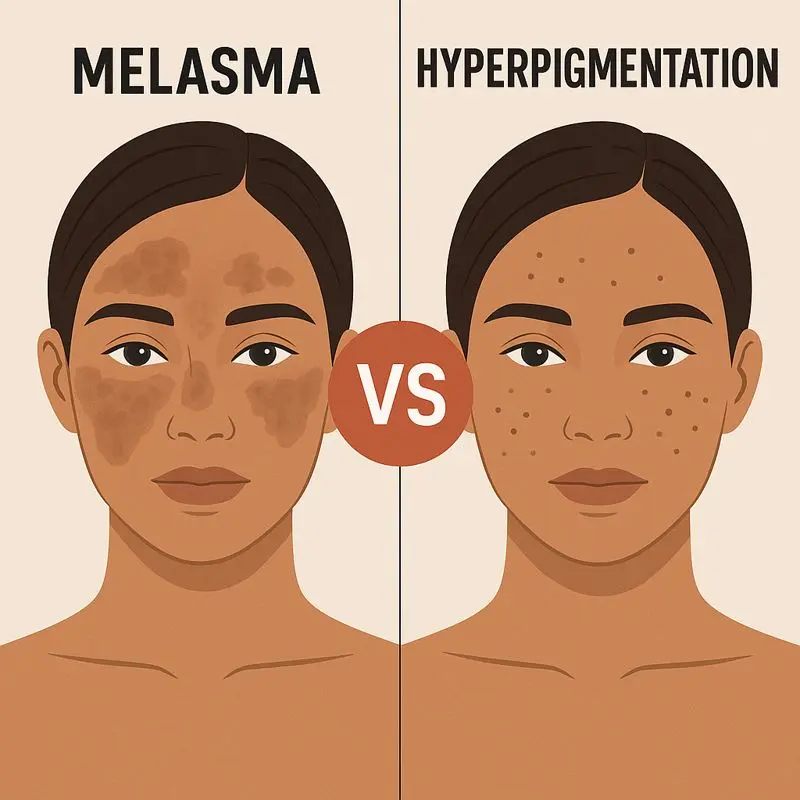
Hyperpigmentation appears as spots or uneven patches. They may be scattered or concentrated but are rarely symmetrical.
Melasma forms large, patch-like areas on both sides of the face. These areas often look like “shadows” or “stains” on the skin.
3. Depth
Hyperpigmentation can be epidermal (surface), dermal (deeper), or mixed. Epidermal PIH responds the fastest to topical treatments.
Melasma often spans both layers. This mixed depth makes treatment more complex.
4. Triggers
Hyperpigmentation triggers:
- UV exposure
- Friction
- Acne
- Skin injury
- Harsh products
- Eczema or irritation
Melasma triggers:
- Hormones
- Heat
- UV exposure
- Pregnancy
- Contraceptive pills
- Genetic predisposition
Melasma flares even from indoor heat sources like cooking or hot showers. Hyperpigmentation rarely reacts this way.
5. Hyperpigmentation Treatment Response
Hyperpigmentation often fades within weeks with:
- Vitamin C
- Azelaic acid
- Retinoids
- Alpha arbutin
- AHA exfoliants
- Sunscreen
Melasma improves slower and requires a gentler, long-term approach. Harsh treatments often worsen it. Heat and sunlight can trigger rebound pigment even after fading.
How to Identify Melasma at Home
You can often recognize melasma by:
- Symmetrical, blurred patches
- Brown, gray, or blue-gray tone
- Appearance on cheeks, forehead, upper lip, or chin
- Sensitivity to heat
- Worsening during pregnancy or hormonal changes
If the pigmentation looks patchy and identical on both sides of the face, there’s a high chance it’s melasma.
How to Identify Regular Hyperpigmentation
Hyperpigmentation is easier to spot:
- Dark spots after acne
- Sun-induced dark marks
- Small concentrated areas
- Uneven tone but not symmetrical
- Spots that darken in the sun
Hyperpigmentation gradually improves when you treat the initial cause and use the right topical ingredients.
What Is PIH and How Is It Different?
Post-inflammatory hyperpigmentation (PIH) is a form of hyperpigmentation that appears after inflammation. Common causes include:
- Acne
- Burns
- Eczema
- Picking at skin
- Infections
- Irritation from harsh products
PIH often appears as brown or purple marks. It’s more common in deeper skin tones due to higher natural melanin production.
PIH is not melasma. It has no hormonal link and responds faster to treatment.
Why Melasma Keeps Coming Back
This is one of your key long-tail keywords, and for good reason. Melasma is known for recurrence.
Here’s why:
1. Hormonal sensitivity
Even small hormonal shifts can activate melanocytes.
2. Heat
Heat—without sunlight—can trigger melasma. Cooking, steam, hot weather, and saunas all increase pigment production.
3. UV exposure
Melasma is extremely UV-sensitive. Even with sunscreen, small amounts of daily exposure can cause flares.
4. Inflammation
Inflammation of any kind (harsh skincare, friction, peeling) can worsen melasma.
5. Chronic behavior
Dermatology research shows melasma behaves like a chronic inflammatory condition. This is why melasma treatment focuses on control rather than permanent removal.
How to Treat Hyperpigmentation Faster
Hyperpigmentation is more responsive to melasma treatment.
Evidence-supported ingredients include:
Topicals
- Vitamin C
- Azelaic acid
- Alpha arbutin
- Niacinamide
- Retinoids
- Glycolic acid
- Tranexamic acid
- Kojic acid
These target melanin production and encourage cell turnover.
Chemical peels
Light AHA or salicylic acid peels help exfoliate pigmented cells.
Lasers
Most hyperpigmentation types respond well to pigment-targeting lasers. However, deeper skin tones need careful settings to avoid worsening the pigment.
Sun protection
Sunscreen is essential. Even a few minutes of UV light can darken PIH and slow progress.
Combining these treatments often leads to faster results, usually within 8–12 weeks.
How to Treat Melasma Safely
Melasma requires a more strategic, slow, and gentle approach.

1. Daily sun protection
Broad-spectrum SPF is the foundation of melasma treatment. Reapplication matters.
2. Heat protection
Avoid peak heat hours. Wear hats. Reduce indoor heat exposure where possible.
3. Topical options
Dermatologists often recommend:
- Azelaic acid
- Tranexamic acid
- Niacinamide
- Low-strength retinoids
- Cysteamine
- Combination creams when appropriate
Vitamin C can help but should be used carefully to avoid irritation.
4. Oral treatments
Low-dose oral tranexamic acid shows promise for stubborn melasma (under medical supervision).
5. Professional treatments
Laser treatment for melasma must be used cautiously. Some lasers can worsen melasma due to heat. Dermatologists typically use gentler devices or avoid lasers entirely for high-risk skin types.
6. Long-term maintenance
Even after melasma improves, maintenance is essential. Without it, melasma often returns.
Melasma vs Hyperpigmentation: Which One Fades Faster?
Hyperpigmentation fades faster because its triggers are easier to control.
Melasma fades slower because hormones and heat continuously stimulate pigment.
Hyperpigmentation typically improves in 2–3 months. Melasma may take several months and requires consistent maintenance to prevent recurrence.
Science-Backed Insights You Should Know
Recent dermatology research reveals:
1. Heat worsens melasma independent of UV exposure.
This is supported by multiple studies highlighting heat-induced melanogenesis.
2. Visible light (blue light) affects pigmentation in deeper skin tones.
Mineral sunscreens with iron oxides offer better visible light protection.
3. Melasma involves vascular and inflammatory components.
This explains why anti-inflammatory ingredients help even when bleaching agents fail.
4. PIH is more common in darker skin.
Melanocytes in skin of color respond more aggressively to even minor inflammation.
These findings guide modern treatment strategies.
Final Thoughts
Melasma and hyperpigmentation look similar, but they behave differently. Knowing which one you have helps you choose the right treatments, avoid irritation, and set realistic expectations.
Hyperpigmentation fades with consistent topical care and sun protection. Melasma improves with gentle treatments, heat control, and long-term maintenance.
Understanding these differences puts you in control of your skin health—and sets the foundation for the next articles in your pigmentation series.
References
- Passeron T., et al. “Melasma Pathogenesis and Treatment Advances.” Journal of the European Academy of Dermatology, 2022–2023.
- Rodrigues M., et al. “Post-Inflammatory Hyperpigmentation in Skin of Color.” Dermatology Research and Practice, 2021–2023.
- Hexsel D., et al. “The Role of Hormones and Heat in Melasma.” Journal of Cosmetic Dermatology, 2022–2024.
FAQS
1. How do I know if I have melasma or hyperpigmentation?
Melasma usually appears as symmetrical patches on both sides of the face, while hyperpigmentation shows up as isolated dark spots from acne, sun damage, or irritation. If your pigmentation darkens with heat or hormonal changes, it is more likely melasma.
2. Which treatment works best for melasma?
Melasma treatment requires gentle, long-term care. Dermatologists often recommend azelaic acid, tranexamic acid, niacinamide, and low-strength retinoids. Melasma can worsen with heat or strong exfoliants, so a controlled routine plus strict sun protection works best.
3. What is the fastest way to fade hyperpigmentation?
Hyperpigmentation treatment responds quickly to ingredients like vitamin C, alpha arbutin, glycolic acid, and retinoids. If the dark spots came from acne or inflammation (PIH), consistent sunscreen use and brightening serums typically show improvement within 8–12 weeks.
4. Why does melasma keep coming back even after treatment?
Melasma is highly sensitive to hormones, heat, and UV exposure. Even small triggers can reactivate melanocytes. This is why dermatologists consider melasma a chronic condition that requires maintenance treatments and daily SPF rather than a one-time cure.
5. Is PIH the same as melasma?
No. PIH (post-inflammatory hyperpigmentation) forms after acne, injury, or irritation, and it fades faster with brightening ingredients. Melasma is hormone-driven, deeper, and more persistent. Treating PIH aggressively may help, but melasma needs a gentler, long-term plan.
Address: Block C, Punjab University Employees Housing Scheme Phase-II, Lahore, Pakistan
Contact Number: +923224563810