Skin Barrier Dysfunction vs Compromised Skin Barrier: What Dermatologists Really Mean
And Why Pigmentation Patients Get Confused
Table of Contents
Introduction: Why This Distinction Matters in Pigmentation
If you’ve ever treated a pigmentation patient whose skin looked healed but continued to darken, relapse, or flare unpredictably, you’ve already encountered the difference between skin barrier dysfunction and a compromised skin barrier — even if the terms were used interchangeably.
In dermatology clinics, these phrases are often casually swapped. In pigmentation-prone skin, especially melasma- and PIH-prone skin, that confusion leads to treatment failure, rebound pigmentation, and chronic inflammation.
This article clarifies:
- What dermatologists actually mean by each term
- Why pigmentation behaves differently in dysfunction vs damage
- How melanocytes respond to barrier signals even after visible healing
- Why correcting pigmentation without addressing dysfunction never works long-term
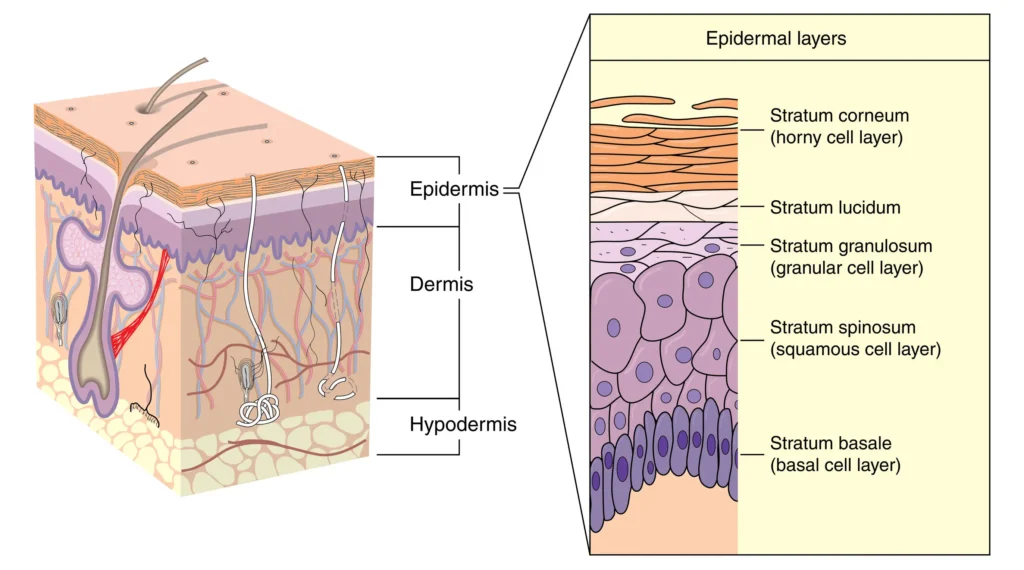
Understanding the Skin Barrier Beyond “Dry or Damaged”
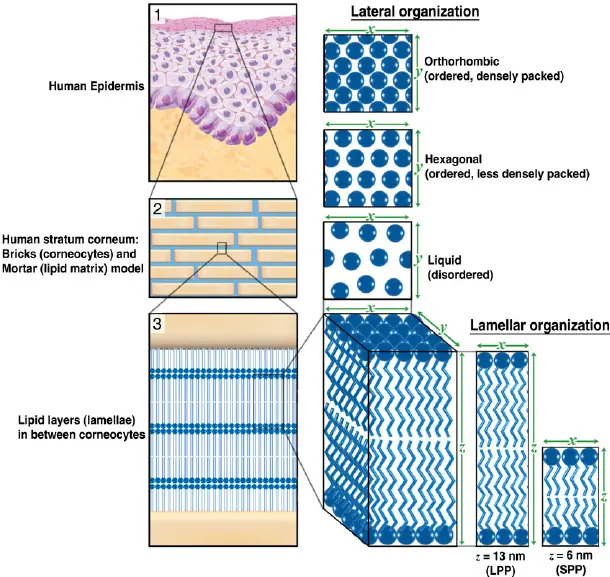
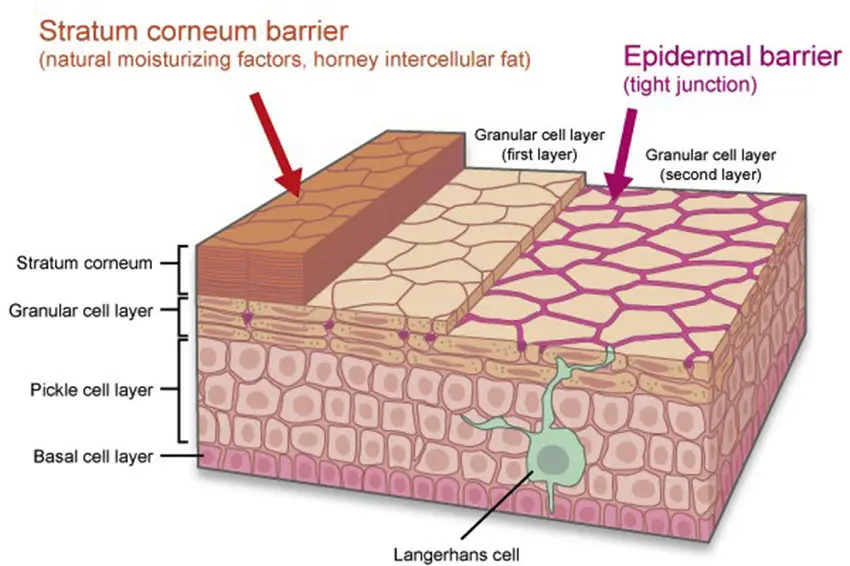
The skin barrier is not just the outermost layer that keeps moisture in. It is a dynamic, immune-responsive system involving:
- Corneocytes (brick cells)
- Lipid matrix (ceramides, cholesterol, fatty acids)
- Tight junctions
- Antimicrobial peptides
- Neuro-immune signaling
- Cytokine regulation
When pigmentation is involved, the barrier also acts as a melanocyte regulator.
Any disruption in this system alters:
- Transepidermal water loss (TEWL)
- Inflammatory mediators
- Melanocyte signaling pathways
This is where damage and dysfunction diverge.
What Is a Compromised Skin Barrier?
A compromised skin barrier refers to structural damage.
Common causes
- Over-exfoliation (acids, retinoids, scrubs)
- Post-procedure skin (microneedling, lasers, peels)
- Harsh cleansers or alcohol-based products
- Acute sunburn or irritant contact dermatitis
Clinical features
- Visible dryness or flaking
- Stinging or burning
- Redness
- Increased sensitivity
- Elevated TEWL
In compromised skin, the barrier is physically broken.
Pigmentation response
- Melanocytes are activated secondarily through inflammation
- Pigmentation often appears after the insult
- With correct repair, pigmentation can improve predictably
Dr. Faiza Shams explains:
“In a compromised skin barrier, pigmentation is usually reactive. If barrier repair is done correctly and early, melanocyte activity often settles.”
What Is Skin Barrier Dysfunction?
Skin barrier dysfunction is not damage.
It is a functional failure of an apparently intact barrier.
This distinction is critical.
Key characteristics
- Skin may look normal or slightly dry
- No obvious peeling or redness
- Patients report “my skin reacts to everything”
- Pigmentation worsens despite gentle care
- Treatments stop working or plateau
In dysfunction:
- The lipid ratio is altered
- Tight junction signaling is impaired
- Immune mediators remain chronically active
- TEWL may be mildly elevated but persistent
Why this matters for pigmentation
Melanocytes respond not only to injury — they respond to inflammatory signaling.
In barrier dysfunction:
- Cytokines such as IL-1α, TNF-α, and PGE2 remain elevated
- Melanocytes stay in a primed state
- Pigmentation continues even without visible irritation
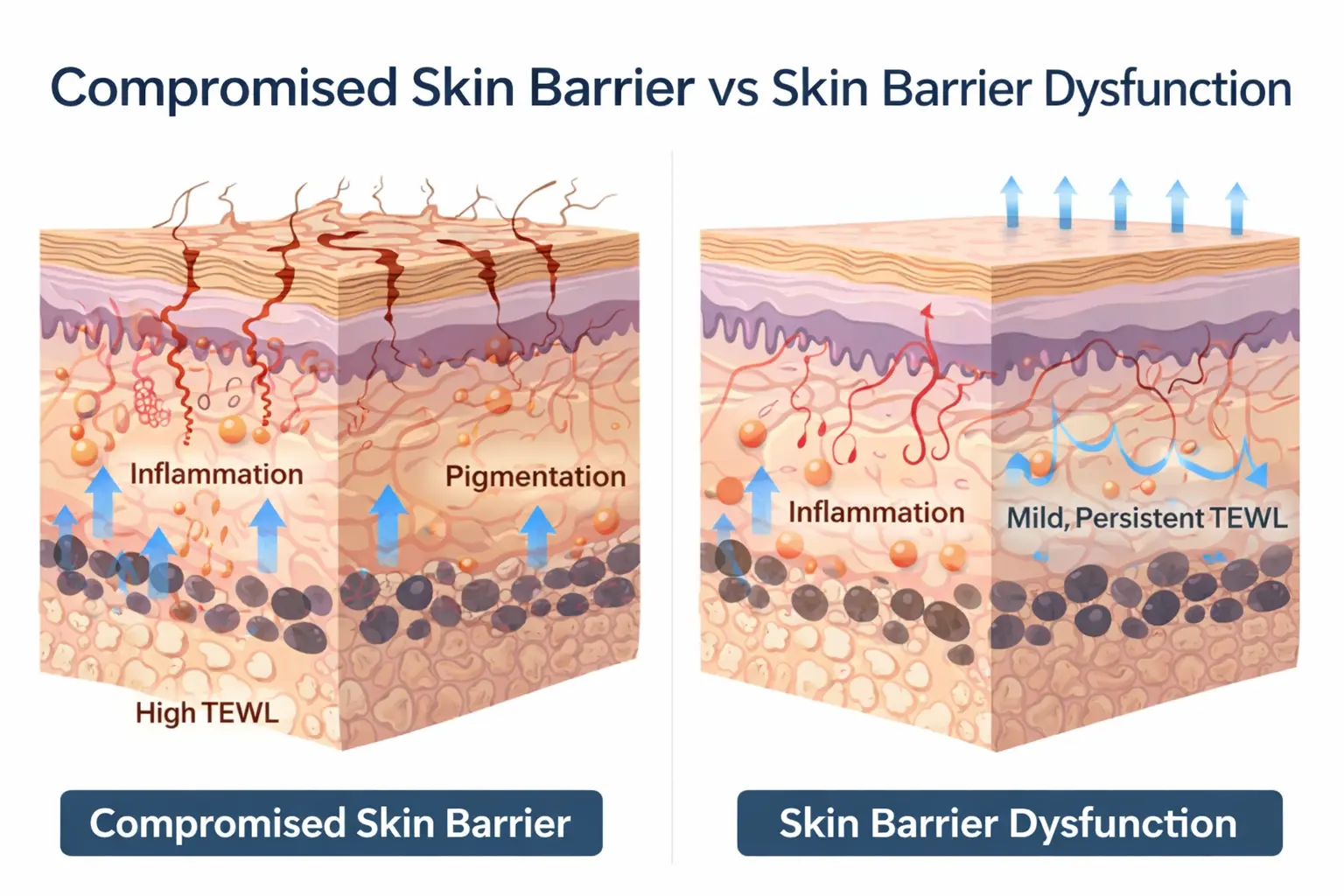
Compromised Barrier vs Barrier Dysfunction: Dermatological Comparison
| Feature | Compromised Skin Barrier | Skin Barrier Dysfunction |
|---|---|---|
| Nature | Structural damage | Functional impairment |
| Visibility | Obvious | Often invisible |
| TEWL | Acutely high | Chronically elevated |
| Inflammation | Acute | Low-grade, persistent |
| Pigmentation | Reactive | Chronic & relapsing |
| Treatment response | Predictable | Inconsistent |
This explains why many pigmentation patients say:
“My skin isn’t irritated anymore, but the pigmentation won’t fade.”
Why Pigmentation Behaves Worse in Barrier Dysfunction
Pigmentation is not only pigment deposition.
It is neuro-immune-melanocytic communication.
In barrier dysfunction:
- The skin sends continuous low-level danger signals
- Melanocytes interpret this as a need for protection
- Melanin production continues even without UV exposure
This is why:
- Melasma relapses without sun
- PIH persists despite lightening agents
- Pigmentation worsens with stress or weather changes
Dr. Faiza Shams notes:
“Barrier dysfunction creates a false alarm state in the skin. Melanocytes keep producing pigment because they believe the skin is under threat.”
The Role of TEWL in Dysfunction-Related Pigmentation
Transepidermal water loss is often discussed but rarely contextualized for pigmentation.
In dysfunction:
- TEWL may not be dramatically high
- But even mild, chronic elevation sustains inflammation
- This perpetuates melanocyte activation
Recent dermatological research shows that persistent TEWL correlates with increased melanogenic cytokines, even when the stratum corneum appears normal.
This explains why:
- Moisturizers alone don’t fix pigmentation
- Barrier “repair creams” fail without functional restoration
Why Standard Pigmentation Treatments Fail in Dysfunction
Common mistakes include:
- Adding more actives when results slow
- Increasing exfoliation for “penetration”
- Switching ingredients repeatedly
In dysfunctional skin:
- Actives penetrate unevenly
- Irritation is subclinical but continuous
- Melanocyte memory strengthens
This aligns with your previously published findings on why pigmentation treatments fail — but here, the mechanism is functional, not product-related.
How Dermatologists Clinically Identify Barrier Dysfunction
Unlike damage, dysfunction is diagnosed through pattern recognition:
- History of repeated flares
- Pigmentation darkening before improvement
- Sensitivity without visible dermatitis
- Seasonal worsening
- Poor tolerance to standard regimens
Advanced clinics may measure:
- TEWL trends
- Corneometry
- Inflammatory biomarkers
But most diagnoses are clinical.
Treating Pigmentation When Dysfunction Is Present
Step 1: Stop chasing pigment
Direct melanocyte suppression without functional repair worsens outcomes.
Step 2: Restore barrier signaling
This includes:
- Correct lipid ratios, not just occlusion
- Anti-inflammatory barrier ingredients
- Neuro-soothing agents
Step 3: Delay aggressive actives
Until:
- Reactivity stabilizes
- Pigmentation stops darkening
- Sensitivity reduces
Dr. Faiza Shams emphasizes:
“In barrier dysfunction, timing matters more than ingredients. Treating too early is worse than waiting.”
Explore barrier-supporting serums for sensitive skin to improve skin stability.
Why This Distinction Changes Long-Term Outcomes
Patients with pigmentation don’t fail treatment because:
- They are non-compliant
- Their skin is “resistant”
- The product is ineffective
They fail because barrier dysfunction is mistaken for healed skin.
Once dysfunction is corrected:
- Pigmentation responds more predictably
- Relapses reduce
- Maintenance becomes easier
Final Takeaway: Damage Heals, Dysfunction Persists
A compromised skin barrier heals visibly.
Skin barrier dysfunction persists silently.
For pigmentation-prone skin, especially melasma and PIH:
- Healing the barrier is not enough
- Function must be restored
- Inflammation must be silenced, not stimulated
Understanding this difference is what separates temporary improvement from long-term control.
FAQ
1. What is the main difference between skin barrier dysfunction and a compromised skin barrier?
A compromised skin barrier refers to visible structural damage, such as peeling, redness, or irritation caused by over-exfoliation, procedures, or harsh products. Skin barrier dysfunction, on the other hand, is a functional problem where the skin appears healed but continues to show sensitivity, inflammation, and pigmentation issues. In dysfunction, melanocytes remain overactive even without obvious irritation, making pigmentation harder to treat.
2. Can pigmentation persist even after the skin barrier looks healed?
Yes. This is common in skin barrier dysfunction. While the surface may look normal, subclinical inflammation and altered barrier signaling can continue to stimulate melanocytes. As a result, pigmentation may persist, darken, or relapse despite good hydration and visible barrier repair.
3. Why do pigmentation treatments fail when barrier dysfunction is present?
Pigmentation treatments often fail because active ingredients are introduced before barrier function is fully restored. In dysfunctional skin, even gentle actives can trigger low-grade inflammation, worsening melanocyte activity. This leads to delayed results, rebound pigmentation, or treatment resistance, despite correct product selection.
4. How long should barrier dysfunction be treated before starting pigmentation actives?
There is no fixed timeline, but pigmentation actives should only be introduced once skin reactivity stabilizes, darkening stops, and sensitivity reduces. Treating pigmentation too early can worsen outcomes. In many cases, prioritizing barrier function for several weeks leads to better and more stable pigmentation improvement later.
Address: Block C, Punjab University Employees Housing Scheme Phase-II, Lahore, Pakistan
Contact Number: +923224563810